Blapherospasm is
the insidious onset of involuntary spasm of muscles affecting eyelid closure.
It is usually bilateral but may be asymmetric and may be associated with some
neurological disorders. Severity may range from mild symptoms to severe
debilitating disease1. Age of onset of blepharospasm is fifth to
sixth decade of life in two-third patients and gradually deteriorates with
time. Females are more affected with 3 to 1 ratio2. Patients may
have risk factors for development of symptoms like a stressful event in life or
problem at work. Sensory tricks can be used by the patients to improve their
dystonia. The most common sensory tricks are touching above the eyes, singing,
talking and humming3. Environmental factors like antipsychotic/ anti-emetic
drugs or history of head trauma can precipitate focal dystonia due to damage to
basal ganglia or cortical/subcortical circuits of brain4.
Hemifacial spasm is a
neuromuscular disease in which unilateral brief or persistent involuntary
contractions occur in the muscles that are innervated by the facial nerve
starting around eyes and then progress to cheek, mouth and neck5,6. Its
prevalence has been estimated at 9.8 cases per 100 000 individuals7.
Different treatment
options like surgical and medical are available for the treatment of blepharospasm
and hemifacial spasm but botulinum neurotoxin injection is the most established
treatment modality8,9. Botulinum neurotoxin A is produced by
clostridium botulinum and is the most potent toxin known to humans. It causes
flaccid paralysis by inhibiting release of acetylcholine from neuromuscular
junction10.
Botulinum
toxin injection gives temporary relief of symptoms and needs to be repeated 3-6
monthly. The purpose of our study is to find out the results of prolonged use
of botulinum toxin injection on its duration of action in patients of blepharospasm
and hemifacial spasm.
MATERIAL AND
METHODS
The study was prospective case series
that was conducted at Yaqin Vision Center, Lahore from Jan 2010 to Dec 2016
after taking ethical committee approval of the hospital. All patients of hemifacial
spasm and essential blepharospasm of both gender and age >25 years were
included in the study. Patients were divided into 2 groups, Group 1 included all patients who had 2-5
injection while group 2 included all patients who had 5-19 injections of botulinum
toxin A (Botox, Allergan). Grouping was done according to the follow up of the
patients. Patients with secondary blepharospasm due to drugs, ocular and
neurological disorders were excluded from the study. In all patients CT
scan/MRI of the brain was done for any facial nerve compression or tumor
involving posterior fossa before injection. Botulinum type A injections were
given after assessing their requirements on the basis of guidelines given by
Jankovic et al2 and severity of blepharospasm as shown in table 1.
Informed consent was taken from all the patients before injection. After taking
standard precautions patients with blepharospasm were injected botulinum type A
at 7 periocular sites on both sides while patients with hemifacial spasm were
injected at 7 periocular and 6-7 perioral sites (orbicularis oris, levator labi,
zygomaticus major, Mentalis and Platysma) as shown in Figure 1. Periocular sites selected were nasally & temporally above the
eye brow, upper lid (pre-tarsal area), lower lid (pre-tarsal area) and one
inferio-lateral to inferior canthus on the orbital rim. Patients were asked
about the onset of effect of Botulinum type A injection and duration of action on
follow up visits. SPSS version 22 statistical package was applied for
descriptive and analytic analysis.
RESULTS
Among forty cases of facial dystonia who got more than one botulinum
toxin A injection, 27 (67.5%) cases were of essential blepharospasm and 13
(32.5%) cases of hemifacial spasm. There were 19 males and 21 females (1:1.1)
with average age of 51 years as shown in Table 2. Total 257 injections were
given to 40 patients with an average of 6.43 injections (range 2-19). Average
51.13 units of botulinum toxin were injected in each injection. Table 3 and
Table 4 shows mean onset & mean duration in Group 1 and Group 2 according
to gender distribution and disease group. Mean onset of action in Group 1 was
3.81 ± 2.6 days and in
Group 2 was 3.92 ± 3.4 days after injection. Mean duration of Botulinum toxin A
efficacy in Group 1 was 3.43 ± 1.5 months and in Group 2 was 3.26 ± 1.6 months. Results of T-test analysis
showed a non-significant p-value of 0.41 for onset and 0.23 for duration of
botulinum toxin A as shown in Table 5.. Figure 2 and 3 show pre-disposing
factors and relieving factors of facial dystonia. Additional factor observed in
the study was effect of weather on symptoms of facial dystonias. 35% cases had
worsening of symptoms in summer while only 2.5% had worsening of symptoms in
winter/cold. Weather had no effect on 62.5% patients with facial dystonias.
Most common complication of botulinum toxin A injection was ptosis in 4.6%.
Other complications included dry eyes in 1.1%, headache in 0.7%, upper lip
droop in 1.5%, upper eyelid bruising in 1.5%, facial deviation in 1.1%, and mild
paralytic ectropion of lower lid in 0.7% of the patients.
Table 1: Grading of severity of blepharospasm.
|
Blepharospasm
severity
|
|
1)
None
|
|
2)
Slight. Increase
blinking in response to external stimulus
|
|
3)
Mild, spontaneous
lid flutter
|
|
4)
Moderate, very
noticeable spasm of eyelids only
|
|
5)
Severe,
incapacitating eyelids and facial muscles spasm.
|
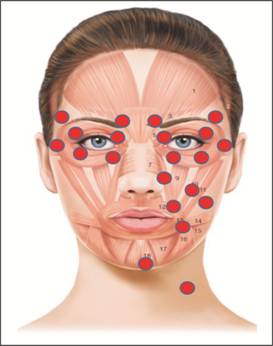
Fig. 1: Sites for Botulinum toxin injection in hemifacial
spasm (Left half of face) and blepharospasm (Right half of face).
Table 2: Mean age of the patients.
|
Facial Dystonia
|
Mean Age (Years)
|
Average
|
|
Male
|
Female
|
|
Blepharospasm
|
53 (n=13)
|
54.86 (n=14)
|
53.96 (n=27)
|
|
Hemifacial spasm
|
46.83 (n=6)
|
43.14 (n=7)
|
44.84 (n=13)
|
|
Average
|
51.05
(n=19)
|
50.95
(n=21)
|
51
(n=40)
|
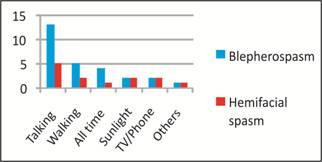
Fig. 2: Predisposing Factors.
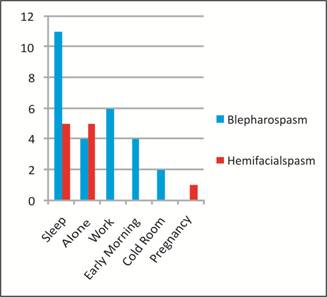
Fig. 3: Relieving Factors.
DISCUSSION
Essential blepharospasm
is an involuntary spasm of eyelid muscles affecting patients in fifth and sixth
decade of life and predominantly affect females than
Table 5: Group 1 versus Group 2.
|
|
Group 1 (n=23)
|
Group 2 (n=17)
|
p-value
|
|
Mean Onset (days)
|
3.81 ± 2.6
|
3.92 ± 3.4
|
0.41
|
|
Mean Duration (months)
|
3.43 ± 1.5
|
3.26 ± 1.6
|
0.23
|
male with 3:12.
It is most common adult-onset dystonia affecting about 16-133 cases per million11.
Hemifacial spasm is unilateral spasm of facial muscle supplied by facial nerve.
It usually affects middle aged people but can present in younger age with
clinical presentation similar to adult onset12.
Botulinum
neurotoxins produced by Clostridium Botulinum cause the disease botulism, in
which prolonged muscle paralysis occurs. In low dose purified botulinum
neurotoxin can be used to treat medical diseases which have uncontrollable
muscle contractions. There are seven different strains A, B, C, D, E, F and G.
A novel in vivo mouse was given botulinum neurotoxins A, B and E which showed
that botulinum A has longer duration of action than botulinum neurotoxin B
while botulinum neurotoxin E had the shortest duration of action13.
In 1989 FDA
approved botulinum toxin A (Botox) for the treatment of strabismus and blepharospasm14.
Later in 2002 it was approved by FDA for frown lines between the eyebrows15.
In 2010 FDA approved Botox for prophylaxis of headaches in adults with chronic
migraines16. Alternate options of botulinum toxin in blpharospasm
are surgical myectomy17 and drugs like tricyclic anti-depressants
and anti-cholinergic18 but these could not get much success and
popularity. Botulinum toxin A (Botox) is available in Pakistan in vial
containing 100 units19. Botulinum toxin is not a cure for focal
dystonias but it gives temporary relief and needs to be injected repeatedly.
Flynn et al20
in their study described that botulinum toxin A (Botox) used for glabellar
lines had a duration of effect for 3-5 months in females and 4-6 months in
males. In a study by Mejia et al21 45 patients of cervical, cranial
and facial dystonias were followed up for a mean of 32 visits and mean of 16
years. There was no significant difference in onset and duration of response to
treatment.
A retrospective
analysis22 of 235 patients of hemifacial spasm, blepharospasm and
cervical dystonia who received botulinum toxin A for ten years showed that
highest response rate at 5 years was similar to response at 2 years. Patient
satisfaction increased after 5 years of treatment with an average benefit of
75.8%.
Hallet23
said that botulinum toxin A injection toxin is distributed by convection and
little diffusion. Toxin uptake depends on activity and temperature. Encouraging
unwanted muscle contraction after injection helps while cooling decreases
uptake. Usually effect of injection finished in 2 months and at 3 months normal
muscle strength returns.
Another study by
Shoaib et al24 showed that after botulinum toxin A (Botox) injection
for blapherospasm and hemifacial spasm onset of action started within 1-2 days.
Mean duration of action was 12.77 +/- 4.68 weeks.
In our study we
gave up to 19 injections with mean onset of injection starting at 3.64 days.
Mean duration of action of a botulinum injection was 3.44 months after which
there was need of repeating botulinum injection. Similar to other studies our
study showed no significant changes in duration of action after prolonged use
of botulinum toxin A injections in cases of blepharospasm and hemifacial spasm
with minimum complications.
CONCLUSION
Botulinum toxin A injection (Botox) is treatment of choice in cases
of facial dystonia as it is safe and shows good efficacy when used in periocular
and facial muscles with minimal complications. It can be used for prolonged
period with consistent results over the years. Careful use of botox injections
can help patients with facial dystonias to live a normal symptoms free life.
Author’s
Affiliation
Prof. Muhammad Moin
FRCS (Edin), FRCOphth
Consultant Ophthalmologist
Yaqin Vision Eye
Center, Lahore.
Dr. Asif Manzoor
FCPS,
Consultant Ophthalmologist,
Yaqin Vision Eye Center, Lahore.
Role of Authors
Prof. Muhammad Moin
Manuscript
design, study design, critical review.
Dr. Asif Manzoor
Data analysis, statistical analysis, manuscript writing.
REFERENCES
1.
Waller RR, Kennedy RH,
Henderson JW Kesty KR. Management of blepharospasm. Trans Am Ophthalmol Soc. 1985; 83: 367–386.
2.
Jankovic J, Orman J. Blepharospasm:
Demographic and clinical survey of 250 patients. Annals of ophthalmology 16 (4): 371-6. May 1984.
3.
Peckham EL, Lopez G, Shamim EA. Clinical features of patients with
blepharospasm: a report of 240 cases. Eur J Neurol. 2011 Mar; 18 (3): 382-386.
4.
Martino D, Defazio G, Abbruzzese G, Girlanda P,
Tinazzi M, Fabbrini G, et al. Head trauma
in primary cranial dystonias: a multicentre case-control study. J Neurol Neurosurg
Psychiatry, 2007 Mar; 78 (3): 260–3.
5.
Rosenstengel C, Matthes M, Baldauf J, Fleck
S, Schroeder H. Hemifacial
spasm conservative and surgical treatment options. Dtsch Arztebl Int. 2012 Oct;
109 (41): 667-673.
6.
Lu AY, Yeung JT, Gerrard JL, Michaelides EM, Sekula
RF, Bulsara KR. Hemifacial spasm and Neurovascular compression.
The scientific world journal. Vol. 2014 (2014), Article ID 349419.
7.
Nilsen B, Le KD, Dietrichs E. Prevalence
of hemifacial spasm in Oslo, Norway. Neurology, vol. 63: 8, 1532–1533, 2004.
8.
Hellman A, Torres-Russotto D.
Botulinum toxin in the management of blepharospasm: current evidence and recent
developments. Ther Adv Neurol Disord. 2015 Mar; 8 (2): 82-91.
9.
Singh S. Botulinum toxin in hemifacial
spasm: Revisited. Indian J Plast Surg. 2013 Jan-Apr; 46 (1): 159-160.
10. Horwath-winter
J, Bergloeff J, Floegel I, Haller-schober EM, Schmut O. Botulinum toxin A treatment in
patients suffering from blepharospasm and dry eye. Br J Ophthalmol. 2003 Jan;
87 (1): 54-56.
11. Valls—Sole
J, Defazio G. Blepharospasm:
Update on Epidemiology, Clinical aspects, and Pathophysiology. Front Neurol.
2016; 7: 45.
12. Tan
EK, Chan LL. Young onset
hemifacial spasm. ActaNeurol Scand. 2006 Jul; 114 (1): 59-62.
13. Keller JE. Recovery from botulinum
neurotoxin poisoning in vivo. Neuroscience,
2006 May 12; 139 (2): 629-37. Epub 2006 Feb 20.
14. Basar
E, Arici C. Use of Botulinum neurotoxin in
ophthalmology. Turk J Ophthalmol. 2016 Dec; 46 (6): 282-290.
15. Nayyar
P, Kumar P, Nayyar PV. A
Singh. Botox: Broadening the horizon of dentistry. J Clin Diag Res. 2014 Dec; 8
(12): ZE25-ZE29.
16. Gooriah
R, Ahmed F. On a botulinum toxin A for chronic
migraine: a critical appraisal. Ther Clin Risk Manag. 2015; 11: 1003-1013.
17. Pariseau
B, Worley MW, Anderson RL.
Myectomy for blepharospasm 2013. Curr Opin Ophthalmol. 2013 Sep; 24 (5): 488-93.
18. Cloud
LJ, Jinnah HA. Treatment
strategies for dystonia. Expert Opin Pharmacother. 2010 Jan; 11 (1): 5-15.
19. Moin
M, Khalid S. Fixed dose botulinum
toxin therapy for blepharospasm. Pak J Ophthalmol 2016, Vol.32 No.2, Apr-Jun,
2016.
20. Flynn
TC. Botulinum toxin: examining duration of
effect in facial aesthetic applications. Am J Clin Dermatol. 2010; 11 (3):
183-99.
21. Mejia N.,
Vuong K., Jankovic J. Long-term
botulinum toxin efficacy, safety, and immunogenicity. Mov.
Disord. 2005; 20: 592–597.
22. Hsiung GYR.,
Das SK., Ranawaya R., Lafontaine AL., Suchowersky O. Long-term efficacy of botulinum toxin A in
treatment of various movement disorders over a 10-year period. Mov. Disord. 2002; 17: 1288–1293.
23. Hallet M. Explanation of timing of botulinum neurotoxin
effects, onset and duration, and clinical ways of influencing them. Toxicon.
2015 Dec 1; 107 (0 0): 64-67.
24. Shoaib KK, Haq
IU, Khan MD. Use of botulinum toxin A
(Botox) in different facial dystonias. J Coll Physicians Surg Pak. 2009 Nov;
19(11): 742-3.